④症例
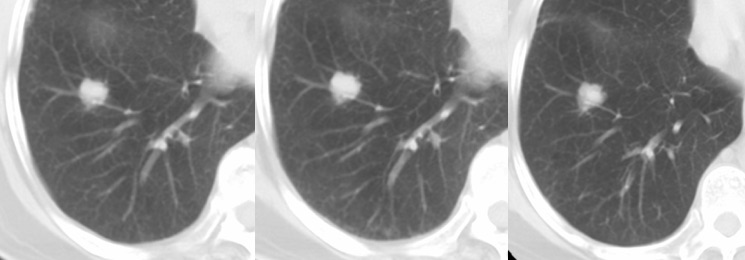
[Case 1]: SPN (solid type)
右下葉A8に接してφ 26mm大のSolid Noduleを認める。周囲にGGOを伴わない辺縁スムースな結節でいわゆる分葉状と表現される結節でありhamartoma(過誤腫)を疑う結節と考えられる。初診時より3年間follow upを行なったがサイズも形状も変化を認めず。左は初診時、中央は2年後、右は3年後のCT画像を示す。
[Case 2]: SSN(Subsolid: part-solid type)
非結核性抗酸菌症(NTIM)に認められた結節性陰影である。右A6末梢にφ8mm大の辺縁にGGOを伴う不均一な結節影を認める。F-18FDGPETCTでは集積像を認めず。3年間follow upを行なったがサイズや形態に変化は認めなかった。1段目は初診時CT、2段目は2年後CT、3段目は3年後CT画像を示す。
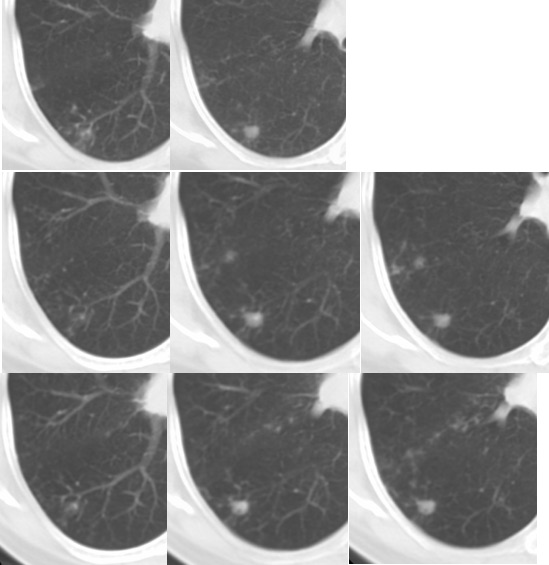
*SSN: subsolid nodule, NTIM: non tuberculous mycobacterial infection
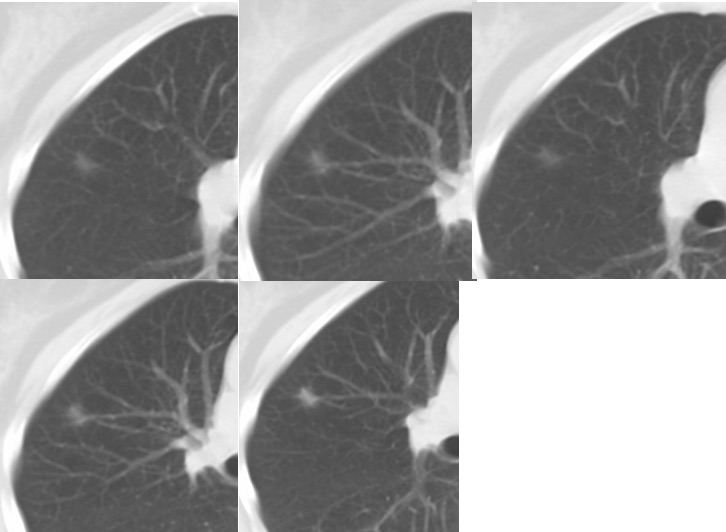
[Case 3]: SSN (Subsolid: pure-GGN type)
慢性咳嗽主訴に来院された際に施行した胸部レントゲン写真で気管支肺炎像を認め、同時に施行した胸部CTで右A4末梢にφ8mm大のすりガラス結節を認めた。右B5末梢のすりガラス陰影(上段の3画像)は、3ヶ月後のfollow up CTで陰影濃度の上昇を認めた。F-18FDGPETCTでuptake亢進を認めVATS(Video-Assisted Thoracic Surgery)による確定診断が行われた。病理診断は、早期肺癌(bronchiolalveolar carcinoma, mucinous type, pT1aN0M0, Stage Ia)であった。
[Case 4]
PFNsと考えられる葉間裂に接した小結節影(粒状陰影)である。①左2つは右上葉胸膜直下の三角形の結節影、②中央二つは左上葉の三角形の結節影、③右二つは右上葉の多角形の粒状影である。①、②は2年間のfollow upで変化なし。③は3ヶ月後のfollow up CTで消失を確認した。

Uploaded on March 03, 2020.
参考文献
1. Elina S, Loprete S, et al. Does aggressive management of solitary pulmonary nodule pay off? Breathe 2019; 15: p15-p23.
2. Raad RA, Suh J, ea al. Nodule characterization Subsolid nodules. Radiol Clin N Am 2014; 52: p47-67.
3. Noguchi M, Morikawa A, et al. Small adenocarcinoma of the lung. Histologic characteristics and prognosis. Cancer 1995; 75: p2844-p2852.
4. Vlahos I, Stefanidis K, et al. Lung cancer screening: nodule identification and characterization. Transl Lung Cancer Res 2018; 7(3): p288-p303.
5. Kikano GE, Fabien A, et al. Evaluation of the solitary pulmonary tumor. Am Fam Physic 2015; 92: p1084-p1092.
6. Hoop BD, Ginneken BV, ea al. Pulmonary perifissural nodules on CT scans: Rapid growth is not a predictor of malignancy. Radiol 2012; 265(2): p611-p616.
7. Qureshi NR, Shah A, et al. Dynamic contrast enhanced CT in nodule characterization: How we review and report. Cancer Imaging 2016; 16(16): p1-p5. DOI 10.1186/s40644-016-0074-4